

Shouldering The Load
By Dr. Nathan Endres
You’re mountain biking and side-slam a tree. You toss a football with friends and one decides to tackle you. You take a short fall while bouldering. Something pops. You can’t move your arm much. Yup, you just dislocated your shoulder.
Shoulder dislocations commonly occur as the result of an injury where the arm is forced away from the body and backwards. It’s usually pretty obvious and yes, this injury is very painful. You may feel like something snapped out of place. You might notice a bulge at the front of your shoulder. You won’t be able to move your arm very much. What do you do?
First, understand what’s happened. A dislocation is when there is complete loss of contact between two joint surfaces. A subluxation is when there is partial loss of contact. In the case of the shoulder, the two surfaces are the humeral head (the ball) and the glenoid (the socket).
The vast majority (more than 90 percent ) of dislocations are anterior (the ball comes out the front). 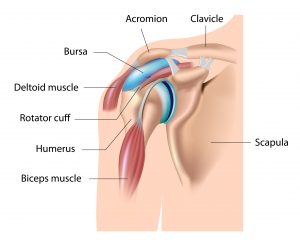 Posterior dislocations definitely happen, but are much less common.
Posterior dislocations definitely happen, but are much less common.
A shoulder separation is a different injury that has nothing to do with the ball and socket. It is an injury to the end of the clavicle (collar bone) where it meets the shoulder blade.
Here are the answers to some of the questions my patients commonly ask:
WHY DO SHOULDERS POP OUT?
The socket of the shoulder is not very deep, so there is not a lot of bony constraint. The ligaments around the shoulder are important stabilizers. The labrum is a ring-like structure around the edge of the socket that’s also very important for stability. It acts a little bit like a wedge under an airplane tire to keep the tire, or in this case, the ball of the shoulder, from moving too far. Muscles around the shoulder, particularly the rotator cuff muscles and muscles around the shoulder blade (rhomboids, trapezius, latissimus) are also important for providing dynamic stability to the shoulder.
If a sufficient force is applied to the shoulder, the static stabilizers of the shoulder (bone, ligaments, labrum) can tear and the shoulder dislocates. Sometimes, this doesn’t require much force, especially if you are loose-jointed to begin with.
WHAT CAN BE DONE TO PREVENT THIS?
Some of it is just luck and avoiding collision sports, like rugby. Otherwise, maintaining really good strength of your dynamic stabilizing muscles may help reduce the likelihood of a dislocation. The keys here are the rotator cuff muscles and the muscles around the shoulder blade. The “beach” muscles like the biceps, triceps and deltoid are less important for shoulder stability.
WHAT DO I DO IF I DISLOCATE A SHOULDER?
The first step is getting it back in place. Sometimes this occurs spontaneously and if it does, you will feel better almost immediately. If this doesn’t happen, the best thing to do is immobilize your arm and get to an emergency room as quickly as possible. Nerve damage can occur when the shoulder is dislocated for a long time. Often, in the emergency department, X-rays will be taken first to confirm the injury. Then the shoulder is put back in place using gentle traction maneuvers, along with sedation and pain medicine.
WHAT GETS DAMAGED WHEN THE SHOULDER DISLOCATES?
Typically, the labrum and ligaments are torn after a shoulder dislocation from an injury. Sometimes, fractures of the ball or socket can occur. In people over 45, it is more common for the rotator cuff to tear after a dislocation. In younger patients, this is not likely. If a rotator cuff tear is suspected, an MRI may be ordered. If a tear is found, surgery is often recommended, as the rotator cuff will not heal on its own and the tear may lead to ongoing pain and weakness.
WHERE SHOULD I GO AFTER THE E.R.?
Follow up with a primary care doctor, orthopaedic surgeon, physical therapist or another sports medicine specialist. It’s probably best to be seen within a week of injury to get a plan together and see if any other testing, like an MRI, is going to be helpful.
HOW ARE DISLOCATIONS TREATED?
Treatment depends on many factors. Age, sex, level of activity and type of sport are all important considerations, as well as whether this was a first-time dislocation, if it happened before, and if there’s a fracture or rotator cuff tear that needs to be addressed. People at the highest risk for recurrent dislocations are young males who play collision sports. So an 18-year-old high school football player may be treated very differently than a 50-year-old who fell skiing.
WILL I NEED SURGERY?
Probably not, but that depends on the factors we just listed. Many people who dislocate their shoulder one time will not have ongoing issues. As you get older, the likelihood of the shoulder dislocating again goes down. Why? For one, your tissues stiffen as you age. Older people are also less likely to participate in collision sports.
HOW DO YOU TREAT A DISLOCATION?
If you do dislocate, your doctor will most likely prescribe a period of immobilization, ice, and anti-inflammatory medication. When the shoulder starts to feel okay, you can get it moving again and then work on strengthening those dynamic stabilizers (rotator cuff and shoulder blade muscles) to decrease the chances of another dislocation. The recovery process may take weeks.
WHY DO PEOPLE NEED SURGERY?
Sometimes there are associated injuries (fractures, rotator cuff tears) that need to be addressed. The most common reason is that the shoulder keeps dislocating again and again, often with less and less force involved. If we think someone is at very high risk for this happening, like our 18-year-old football player, we may recommend surgery after just one dislocation.
WHAT IS THE SURGICAL TREATMENT?
That gets complicated. The most common surgery is called a “Bankart repair.” Bankart was a surgeon who described the labral tear, often seen with a shoulder dislocation. This was in the 1930s. A Bankart repair involves reattaching the torn labrum back to the socket with anchors. This can be done in an open fashion or through minimally invasive arthroscopic techniques. When somebody has had multiple dislocations, there is often bone loss that occurs on the ball and/or socket. If this is the case, a Bankart repair is less successful and other procedures that address the bone loss may be a better option.
ARE THERE ANY LONG-TERM ISSUES?
One concern is that the shoulder is going to dislocate again. The likelihood of that depends on evaluating the risk factors we talked about earlier. The other long-term concern is arthritis which has been associated with repeated dislocations.
Dr. Nathan Endres is an orthopedic surgeon at the University of Vermont Medical Center. He specializes in sports medicine and fracture treatment. He is a team physician for the University of Vermont, St. Michael’s College and the U.S. Ski Team.
